
What Your MRI Actually Means (And What It Doesn’t)

Getting an MRI is almost always a scary experience. It usually means you’re having some kind of pain and you’re trying to figure out what is going on. Once you finally get the MRI back there might be a list of things that show up on it. When you google those findings you’ll often see discussion about injections or surgery that will be necessary to feel better. While MRIs are an important diagnostic tool, they don’t always tell the whole story as to why you may be having pain.
The Core Problem With MRI Interpretation
An MRI is great for figuring out structural issues that require immediate attention. Some of these things might be disc herniations with progressive numbness and weakness in your legs or an ACL tear. These things are unlikely to get better on their own and it is important to diagnose them so you can figure out the next best treatment. What they are probably less effective for is pain that has been lingering at a low level for a long time. In this situation getting an MRI is likely going to show a bunch of things that may or may not be related to your pain. Some of these findings are just more prevalent over time. You can think of them as internal signs of aging like a grey hair or wrinkle. While no one loves to have them, it doesn’t necessarily mean that something is wrong.
What Asymptomatic People Actually Look Like on MRI
The reason that we think these findings are normal with aging is that research has shown these findings also show up in people without any pain at all. If there was a 1:1 correlation between imaging and pain we should expect every person with MRI findings to have the same pain but this just isn’t the case. A large systematic review of low back imaging found that 68% of people with no symptoms over the age of 40 had disc degeneration and 50% showed disc bulges¹. Separate research on the cervical spine found that 20% of people without pain had findings of spinal cord compression in their neck². When pooling data across shoulder studies, the occurrence of a full thickness rotator cuff tear in people with no pain in their shoulder ranged from 0-14% depending on the population studied³. A systematic review looking at knee MRIs showed features of osteoarthritis in 19-43% of adults over the age of 40 without knee pain. The likelihood of finding OA-related features increased approximately 10-15% per decade⁴. A study of 45 participants without pain in their hip underwent MRI and labral tears were seen in 69% of hips and people over the age of 35 were significantly more likely to demonstrate joint defects associated with OA⁵. It is important to keep this in mind when reviewing your own MRI results, as the findings that show up are not always the whole picture as to why pain is occurring.
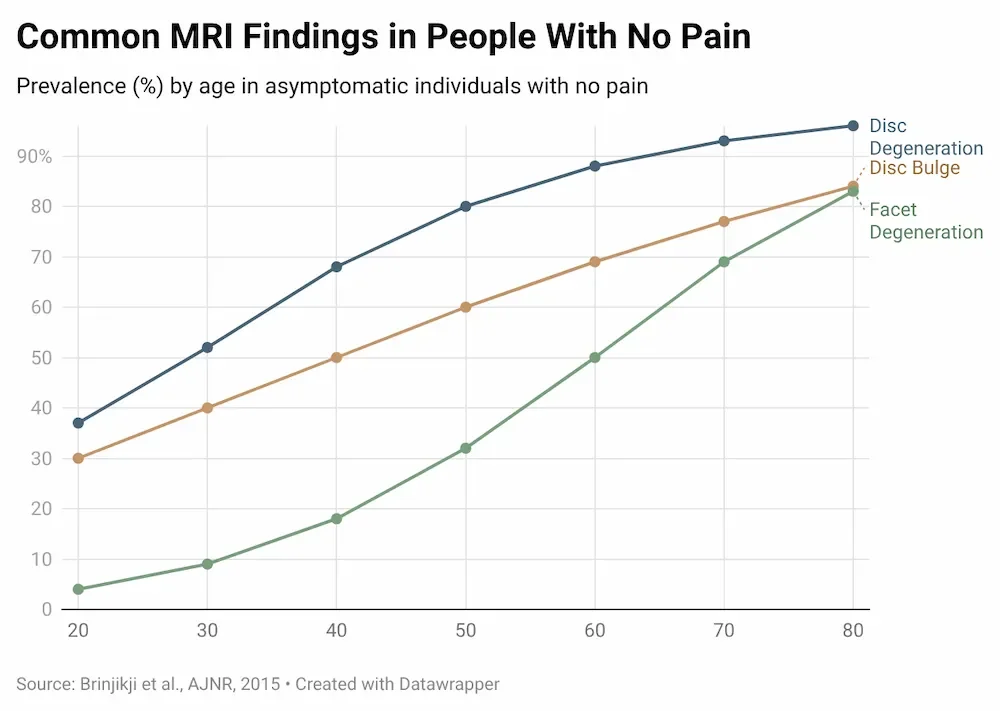
Prevalence of common MRI findings in people with no pain, by age. Brinjikji et al., AJNR 2015.
Does This Mean MRI Is Useless?
It is important to not throw the baby out with the bath water here as MRI still can be incredibly important for diagnosing a variety of conditions. MRI is excellent at determining issues with internal organs, diagnosing tumors, and traumatic injuries like a ligament tear. While MRI isn’t the best for determining causes of long standing lower levels of orthopedic pain it is very helpful for more serious pathologies that are important to rule out. If your doctor is concerned that your pain could be due to something more concerning then an MRI is a great tool to rule it out. The issue arises when MRI findings are used to confidently claim things about lower levels of pain that appear to come from a joint or muscle.
So What Does Cause Pain?
While many people think of pain as what happens when some part of their body is damaged, it is actually much more complex than that. A very brief summary of the pain pathway is that nerve endings register a stimulus and that signal then goes through the spinal cord up to the brain. The brain then determines whether that stimulus is intense enough to create the perception of pain. This means that past experiences, current emotional state and more can determine whether the brain actually decides that the stimulus it receives is a painful one. We see how structure alone is not the cause of pain because MRI changes do not always accompany pain changes. This systematic review looked at people who had undergone rotator cuff repair due to a torn tendon. In this study 30% of asymptomatic people actually had re-torn their tendon⁶. So even though they still had the same diagnosis that initially prompted surgery, they were satisfied with their outcome and no longer had pain. Another study followed people already diagnosed with knee osteoarthritis and performed repeat MRI. The findings showed that people’s pain and function did not correlate well with increasing signs of osteoarthritis on imaging⁷. We can see that the sensation of pain is much more complex than just what shows up on an MRI report.
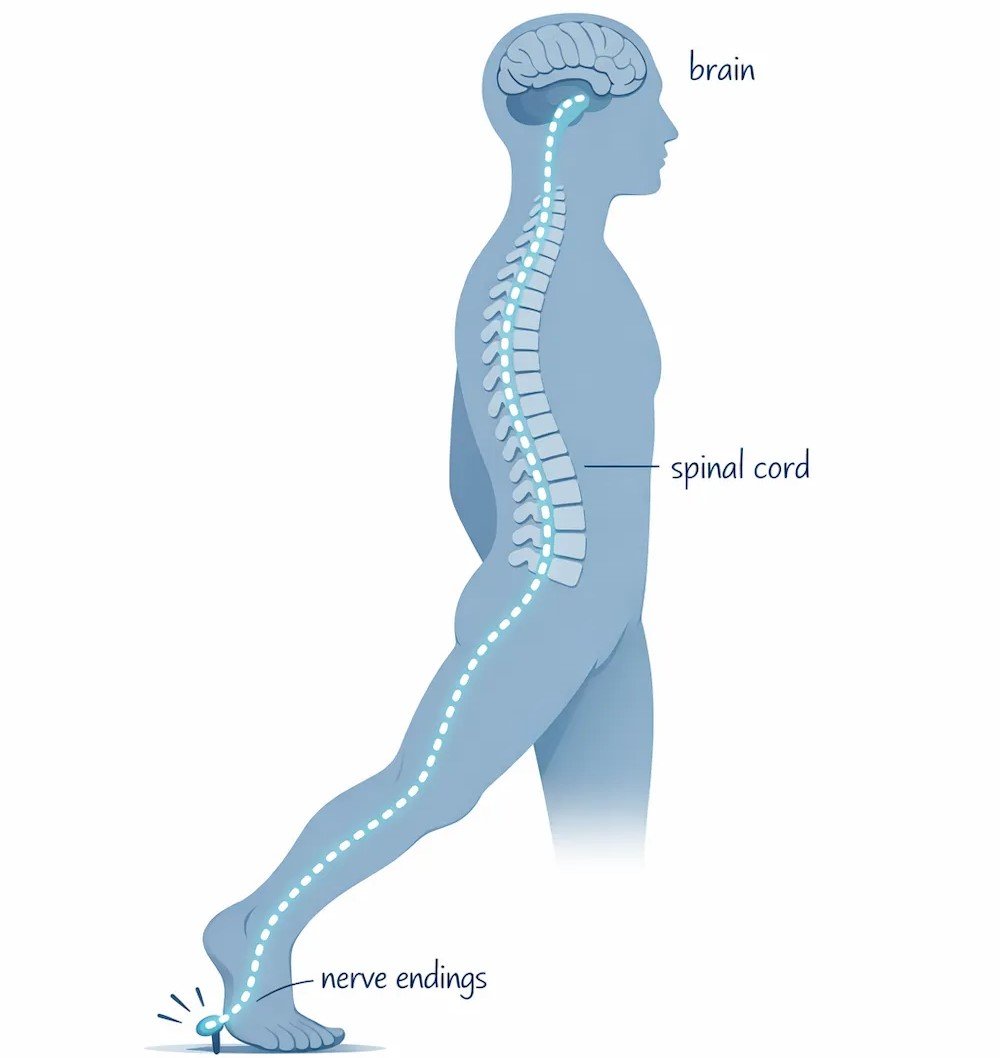
A simplified pain pathway. Nerve signals travel from the body through the spinal cord before the brain determines whether to create the sensation of pain.
What To Do With Your MRI
Now if you already have an MRI and you’re concerned about the findings, here are the next steps I’d take. Assuming it is for an orthopedic problem like we discussed, it is always a good idea to ask your doctor or orthopedic specialist their thoughts on it and whether it warrants surgical intervention. If that is not the case, then the great news is that it is likely something you can try conservative treatment for like physical therapy, massage, acupuncture etc. The most important thing to keep in mind is that the MRI findings are not a life sentence. For example, those with lumbar disc bulges and herniations actually show spontaneous reabsorption of disc material with more severe cases being the most likely to reabsorb⁸! Imaging findings are one aspect of what might be causing your pain and it is important to consider all other factors as well to have the most successful outcome in your rehab. If you’re feeling stuck with pain or have MRI findings that you want to discuss please reach out and book a call with me and I’d be happy to help.
Sources:
Brinjikji, W., Luetmer, P. H., Comstock, B., Bresnahan, B. W., Chen, L. E., Deyo, R. A., Halabi, S., Turner, J. A., Avins, A. L., James, K., Wald, J. T., Kallmes, D. F., & Jarvik, J. G. (2015). Systematic literature review of imaging features of spinal degeneration in asymptomatic populations. AJNR. American journal of neuroradiology, 36(4), 811–816. https://doi.org/10.3174/ajnr.A4173
Smith, S. S., Stewart, M. E., Davies, B. M., & Kotter, M. R. N. (2021). The Prevalence of Asymptomatic and Symptomatic Spinal Cord Compression on Magnetic Resonance Imaging: A Systematic Review and Meta-analysis. Global spine journal, 11(4), 597–607. https://doi.org/10.1177/2192568220934496
Sanders, S., Ibounig, T., Haas, R., Jones, M., Rämö, L., Docking, S., Järvinen, T., Taimela, S., Hoffmann, T., & Buchbinder, R. (2025). Rotator Cuff Imaging Abnormalities in Asymptomatic Shoulders: A Systematic Review. The Journal of orthopaedic and sports physical therapy, 55(12), 1–16. https://doi.org/10.2519/jospt.2025.13611
Culvenor, A. G., Øiestad, B. E., Hart, H. F., Stefanik, J. J., Guermazi, A., & Crossley, K. M. (2019). Prevalence of knee osteoarthritis features on magnetic resonance imaging in asymptomatic uninjured adults: a systematic review and meta-analysis. British journal of sports medicine, 53(20), 1268–1278. https://doi.org/10.1136/bjsports-2018-099257
Register, B., Pennock, A. T., Ho, C. P., Strickland, C. D., Lawand, A., & Philippon, M. J. (2012). Prevalence of abnormal hip findings in asymptomatic participants: a prospective, blinded study. The American journal of sports medicine, 40(12), 2720–2724. https://doi.org/10.1177/0363546512462124
Davey, M. S., Hurley, E. T., Carroll, P. J., Galbraith, J. G., Shannon, F., Kaar, K., & Mullett, H. (2023). Arthroscopic Rotator Cuff Repair Results in Improved Clinical Outcomes and Low Revision Rates at 10-Year Follow-Up: A Systematic Review. Arthroscopy : the journal of arthroscopic & related surgery : official publication of the Arthroscopy Association of North America and the International Arthroscopy Association, 39(2), 452–458. https://doi.org/10.1016/j.arthro.2022.11.002
Phan, C. M., Link, T. M., Blumenkrantz, G., Dunn, T. C., Ries, M. D., Steinbach, L. S., & Majumdar, S. (2006). MR imaging findings in the follow-up of patients with different stages of knee osteoarthritis and the correlation with clinical symptoms. European radiology, 16(3), 608–618. https://doi.org/10.1007/s00330-005-0004-5
Rashed, S., Vassiliou, A., Starup-Hansen, J., & Tsang, K. (2023). Systematic review and meta-analysis of predictive factors for spontaneous regression in lumbar disc herniation. Journal of neurosurgery. Spine, 39(4), 471–478. https://doi.org/10.3171/2023.6.SPINE23367